Is Africa on the verge of another virulent attack of the dreaded Ebola virus? This time, it is the Bundibugyo Ebola strain, different from the Zaire Ebola of 2014. Is the Bundibugyo Ebola potentially more dangerous than the Zaire Ebola that took the lives of courageous Dr Ameyo Adadevoh, OON, other medical practitioners and a number of other Nigerians in 2014? Questions that should agitate the minds of concerned Nigerians are, how dangerous the Bundibugyo Ebola is, particularly as so far, there’s no vaccine for it or cure? Why does Ebola appear to originate from the Democratic Republic of Congo (DRC)? How prepared is Nigeria, and Lagos in particular, being one of the major gateways into Nigeria, to tackle and contain the virus? How should people protect themselves from contracting the virus? Onikepo Braithwaite and Jude Igbanoi sought out the Director, Epidemiology, Biosecurity and Global Health/State Epidemiologist, Lagos State Ministry of Health, Dr Ismail Abdus-Salam to tease out the answers to these questions, particularly about symptoms that people should be aware of, and what steps should immediately be taken, if there’s suspicion that an individual may have contracted the virus
Guarding the Gateway: Lagos, and the Bundibugyo Ebola Threat
You are the Director of Epidemiology, Biosecurity and Global Health at the Lagos State Ministry of Health. Kindly, give us a brief overview of what this role entails, vis-à-vis communicable diseases.
Thank you. In simple terms, my department is the State’s early-warning system and first organised line of defence against disease. Lagos is the most populous, most connected sub-national entity in West Africa — over twenty million people, an international airport, two seaports and busy land approaches. Pathogens move with people and goods, so our job is to see a dangerous disease early, contain it, and limit harm.
That work rests on a few pillars: surveillance — analysing data from hospitals, laboratories, communities and points of entry, so an unusual cluster is flagged within days; preparedness and response — our emergency operations centre, rapid response teams, and isolation and case-management capacity; and biosecurity at our borders with the Port Health authorities. Cutting across these are laboratory diagnosis, contact tracing, infection control and risk communication.
On communicable diseases, we work under the National Integrated Disease Surveillance and Response framework and closely with the NCDC, watching Lassa fever, cholera, measles, mpox and now Ebola. The principle is the same for all: detect early, isolate, treat, trace contacts, engage the community. A disease caught at one or two cases is a manageable incident; at fifty, it is a crisis.
Since the 2014 Zaire strain Ebola outbreak, we have heard of other outbreaks in the Democratic Republic of Congo (DRC). Reports suggest hundreds of cases and dozens of deaths in this 2026 Bundibugyo outbreak, which has spread to Uganda. What is the suspected source, and how does the Bundibugyo strain differ from the Zaire strain of 2014?
First, an accurate picture, because the statistics changes daily. The DRC declared the outbreak on 15 May, 2026 after confirming Bundibugyo virus in Ituri Province — the 17th Ebola outbreak there since 1976. The WHO declared a Public Health Emergency of International Concern on 16–17 May, the Africa CDC, a Continental emergency the next day. By early June, the affected countries reported several hundred cases and well over a hundred deaths, still confined to the DRC and Uganda, with imported cases — including health-worker deaths — in Kampala.
On the source: Ebola is zoonotic. The reservoir is believed to be fruit bats, with primates and other forest animals as intermediate hosts; the first human infection follows contact with an infected animal in forest or hunting settings. Genetic sequencing confirms this is a fresh spillover, not the re-emergence of an old outbreak.
Now the crucial difference. “Ebola” is not one virus, but a family. The Zaire strain that reached Nigeria in 2014, is historically the deadliest — case-fatality rates of 40% to 90%. The Bundibugyo strain, first identified in Uganda in 2007, has been less lethal historically — roughly 25%-50% — though this outbreak’s early figures are provisional. But, lower fatality does not make it less serious: our tools were built for the Zaire strain, and Bundibugyo is genetically distinct, its key surface proteins differing by roughly 30%.
Ervebo, and the treatments Inmazeb and Ebanga, all target the Zaire virus, and are not expected to protect reliably against this strain. So, the world relies on classic methods — finding and isolating cases, tracing contacts, safe burials, early care — not a proven vaccine or cure. That is the defining feature of 2026.
Exactly how is Bundibugyo Ebola transmitted from person to person? Can it spread through the air or casual touch, or must it be through the body fluids of those who are ill?
Let me be direct: misunderstanding here causes needless panic. Ebola is not airborne. It does not spread like flu or Covid-19; you cannot catch it by sharing air or passing someone on the street.
Transmission requires direct contact with the blood or body fluids of a person already sick with Ebola, or who has died of it, entering through broken skin or the mucous membranes of the eyes, nose or mouth, or via surfaces soiled by those fluids.
Two essentials. A person infected, but not yet symptomatic, is not contagious; people become infectious, only once ill. And, the body of someone who has died of Ebola is highly infectious, which is why traditional washing of the dead has driven so much transmission — safe burials by trained teams are vital. So, plainly: casual contact poses no meaningful risk; the danger is close contact with the fluids of the visibly sick and the dead — hence, caregivers and health workers are most at risk.
What safety measures should people take to avoid contracting the virus? Is there any approved vaccine or preventive treatment for Bundibugyo Ebola?
Because the routes of transmission are well understood, the measures are practical. Avoid the blood or body fluids of anyone unwell with fever; never handle the body of someone who has died of a suspicious illness; practice rigorous hand hygiene; and avoid bushmeat, especially bats and primates, and sick or dead wild animals. If fever follows contact with a sick person or travel to an affected area, call the authorities rather than moving from clinic to clinic, and do not self-medicate.
On vaccines and treatment, I must be candid. There are no licensed vaccines and no specific approved medicine for the Bundibugyo strain. Ervebo is licensed only against the Zaire strain, and because the two viruses differ in their key surface proteins by roughly 30%, it is not expected to protect reliably against this one. Newer candidates are being researched, but remain early and investigational.
So, prevention and early care carry the weight of survival: even without a specific drug, early supportive care — fluids, oxygen, treating co-infections, good nursing — saves lives, and a patient who presents early fares far better than one who hides at home until too late.
What is the incubation period from exposure to symptoms? What early symptoms should people watch out for, and how do they differ from Malaria and Flu? What must someone who suspects they have Ebola do, especially in a family setting?
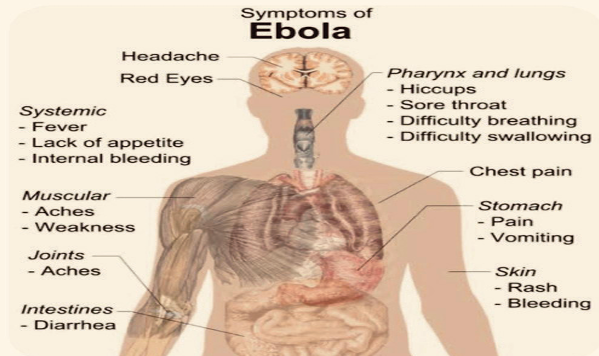
The incubation period — exposure to first symptoms — is 2 to 21 days, most often 8 to 10, which is why contacts are monitored for a full 21 days. The early symptoms are non-specific: sudden fever, weakness, headache, muscle pain, sore throat, then vomiting and diarrhoea. Bleeding, which most associate with Ebola, is actually a later and not universal feature.
Telling it apart from Malaria and Flu is hard: in the first day or two you often cannot, and that is the danger. Fever and body aches describe Malaria, Typhoid, Lassa Fever and early Ebola alike, and in Nigeria the likely cause is often Malaria. So, the differentiator is not the symptom, but the context — recent travel to or from an affected area, or contact with someone sick or dead from a fever. Always test promptly for Malaria, but if such a history accompanies the fever, treat it as a possible viral haemorrhagic fever and call for help. Diagnosis is harder here: the standard rapid test, built for the Zaire strain, does not reliably detect Bundibugyo, so confirmation needs specialised assays.
What should the individual suspected to have Ebola do? Do not board public transport or sit in a crowded clinic. Isolate in a separate room, and immediately call the State emergency lines — 767 or 112 — or the NCDC line, 6232.
In a family setting, designate one healthy adult caregiver who uses gloves and protective covering, and washes hands meticulously; do not share plates, cups or bedding; keep visitors away. If someone dies, do not prepare the body — call the emergency line, so a trained team can conduct a safe, dignified burial.
Is there synergy among the States in handling communicable diseases? Does the NCDC play a pivotal or central role in State-level arrangements?
Yes — one of the genuine success stories of Nigerian public health, since 2014. Disease does not respect State boundaries, so our response cannot be fragmented, and it is not.
The NCDC is the national coordinating body, and its role is central: it sets the guidelines every state uses, runs the national reference laboratories and emergency operations centre, deploys rapid response teams, and issues the advisories driving our posture. In late May, it classified Nigeria’s importation risk as high and named Lagos among ten high-risk States required to scale up surveillance, laboratory readiness and isolation — a single advisory that aligned the Federation within days.
But, this is a partnership, not top-down command. The States are the operational frontline: we run our own emergency operations centre, surveillance and laboratory systems and isolation facilities, feed data upward, and draw on national resources when an event exceeds us. We also coordinate with neighbours — Ogun in particular — and through a One Health approach with the agriculture, environment, education and environmental-protection agencies. The NCDC is the conductor, the States the orchestra, playing from the same score.
Some say Nigeria should close its doors to the DRC and Uganda, since there is no treatment. A Spanish Mayor has reportedly banned the DRC from a pre-World Cup match. Isn’t closing the borders the sensible thing to do — prevention being better than a cure that does not exist?
I understand the instinct — when people hear “no cure”, the reaction is to pull up the drawbridge. But, the considered public-health position is different. The WHO, under the International Health Regulations, advises against general travel and trade bans, and does so again in 2026. Blanket closures are largely ineffective — people find informal routes across porous borders — and counter-productive: they push movement underground, discourage honest reporting, cripple economies, and breed stigma, as we saw in 2014.
What works is targeted vigilance, which Nigeria has deployed: enhanced screening at points of entry, exit screening, and follow-up of arrivals for 21 days, under a Federal entry protocol issued in late May.
On the Spanish case — the Mayor of La Línea cancelling the DRC’s 9 June friendly against Chile — footballers are not patients. The squad has trained in Belgium under strict protocols, with isolation required before the World Cup; a healthy, screened, asymptomatic team poses negligible risk. Such decisions reflect public anxiety, more than epidemiology. Prevention is paramount — but done properly, it is surveillance, screening, preparedness and trust, not isolationism we know fails.
Has Lagos State upgraded its isolation facilities since the Covid-19 pandemic in 2020? And, what is your assessment of the Nigerian medical community’s level of preparedness to tackle this unpredictable ‘second coming’ of Ebola — especially since many of Nigeria’s best medical personnel are said to have ‘japaed’, migrating abroad in search of greener pastures?
Significantly, yes. If 2014 taught Lagos to take infectious disease seriously, 2020 taught us to invest at scale. We describe our framework as a biosecurity “bio-shield” — a permanent culture of readiness, tested in 2014, strengthened through Covid-19, and exercised continuously against Lassa fever and Cholera. At its apex sits the Lagos State Incident Command System, led by Mr Governor as Incident Commander, while our Emergency Operations Centre runs around the clock.
On facilities: the Lagos Mainland Hospital in Yaba — our Infectious Disease Hospital, which managed Nigeria’s Ebola index case in 2014 and was expanded during Covid-19 — is on high alert, with triage, isolation wards, intensive care and specialists. Its on-site Biosafety Level-3 laboratory and Biobank let us confirm samples here, not wait, as in 2014.
Readiness, though, is systems and people. In recent weeks we held a high-level coordination meeting with the Commissioner for Health, the Special Adviser, the Permanent Secretary and pillar leads; circulated an Ebola fact sheet to health workers and community leaders; sensitised all twenty-three disease surveillance and notification officers; and ran training-of-trainers for public and private facilities — ‘private’ deliberate, because a private hospital first received Patrick Sawyer in 2014. We have drawn community health workers and civil-society groups into our early-warning network, and pre-positioned protective equipment.
I also joined a preparedness inspection of the Murtala Muhammed International Airport, our most critical gateway, which carries roughly 70% of the country’s international passenger traffic. With Port Health, FAAN and others, we reviewed screening, infection control and isolation; touchless sanitiser dispensers and temperature-detection are deployed, and dedicated channels for high-risk arrivals are being explored. The aim, as the Commissioner put it, is a bottleneck for the virus, not for passengers; flights from East and Central Africa now get heightened scrutiny.
On national preparedness, my candid view is that Nigeria is far better prepared than in 2014. The NCDC now runs molecular laboratories, emergency operations centres and an incident-management system absent in 2014; we contained Ebola in 2014, weathered Covid-19, and manage Lassa fever — a viral haemorrhagic fever — every year, so the muscle memory is real.
I will not pretend we have no weaknesses: the migration of health workers you call ‘japa’ is a genuine strain, especially on nurses and specialists. But, outbreak response rests on systems, protocols and a trained core, not any single individual — and such a system is what we are building.
That is why we invest continuously in training. Only weeks ago, we ran a three-day workshop on case management for priority diseases — covering mpox, diphtheria and viral haemorrhagic fevers, the category that includes Ebola — for case managers from public and private facilities, with partners including the FHI 360-led EPIC project and the United States Department of State. It was designed to cascade, so those we train teach others. We reach the private sector through the Health Facility Monitoring and Accreditation Agency, because every Facility must be ready.
The reassurance Lagosians most want: to date the State has recorded no suspected or confirmed case, and our task is to keep it that way — with vigilance, not alarm.
We cannot speak of Ebola in Nigeria without remembering the late Dr Ameyo Adadevoh, OON, who died after caring for Patient Zero, Patrick Sawyer. This time, what plans are in place to protect medical practitioners from contracting the virus from their patients — and what level of sensitisation do Nigerian practitioners have about this dangerous virus and how to handle it?
I am glad you raised her name, because she must never be forgotten. Dr Ameyo Stella Adadevoh and the colleagues who died alongside her, almost certainly saved this country in 2014: she recognised the danger, refused under pressure to discharge Patrick Sawyer, and contained the index case. Protecting health workers today, is honouring her.
The hard fact is that in 2014, and in the DRC and Uganda now, health workers have been among the first victims — almost always because the patient was not suspected of Ebola, and was treated as an ordinary fever case until too late. The single greatest protection, is early suspicion.
Our plan operates on layers. Screening and triage begin at the facility entrance, so a patient with a suggestive history is separated before reaching a crowded ward. We enforce strict infection prevention and control — dedicated teams, protective equipment, and supervised donning and doffing, since removing contaminated gear is when many infections occur. We have extended training to private as well as public facilities and maintain isolation pathways. And, the diagnostic difficulty I mentioned makes a clinician’s index of suspicion more important than ever.
You ask how well sensitised our practitioners are. In a sector as vast as ours the picture is uneven, and sustaining awareness across every clinic is the standing challenge. But, it is what we are working at: the fact sheet circulated to practitioners; the recent case-management training covering viral haemorrhagic fevers, built to step down to many more; and continuous infection-prevention drills. The 2014 generation learned this at terrible cost; our duty is to ensure the current generation learns it in the classroom, not on the ward.
One sober point: because there is no proven vaccine for the Bundibugyo strain, we cannot give frontline staff the vaccine shields available against the Zaire strain, which makes discipline around protective equipment decisive. We will not ask them to stand in the breach without the equipment, training and support Dr Adadevoh’s generation too often lacked.
Are there long-term effects for survivors? In 2014, survivors were asked to abstain from sexual activity for a period, as the virus persists in the body after recovery. What are the current injunctions?
Yes — and this deserves far more understanding and compassion than it usually receives. Surviving Ebola is a triumph, but not always the end of the story. Many survivors experience post-Ebola syndrome: persistent joint and muscle pain, fatigue, headaches, and eye inflammation that, untreated, can progress to blindness. Beyond the physical, there is a heavy psychological toll — anxiety, depression, post-traumatic stress — worsened by stigma.
Your point about persistence is medically important. After a patient clears the virus from the bloodstream, it can linger for months in protected sites — most notably the semen of male survivors, and also the eye, central nervous system and breast milk — creating a real, if limited risk, of sexual transmission.
Following WHO guidance, male survivors are counselled to practice safer sex — abstaining or using condoms — until their semen tests negative twice; absent testing, the historical guidance is around twelve months. Breastfeeding survivors receive specific guidance on their milk. And, all survivors should have structured follow-up, combining medical monitoring with mental-health support.
One honest caveat: much of this data comes from Zaire-strain survivors; persistence is presumed similar for Bundibugyo but less characterised, and guidance will be refined as the science matures. The principle does not change: a survivor deserves care, follow-up and dignity — not fear and exclusion.
To close: Ebola is dangerous, but not mysterious — we know how it spreads, and how to stop it. Our strongest instruments are early reporting, basic hygiene, accurate information and public trust. Lagos is vigilant, our systems active, and with the public’s cooperation, we are ready.
Thank you Dr Abdus-Salam.


